Has the Supreme Court changed DoLS? What the 2026 ruling really means for care providers, managers and leaders
There has been a lot of discussion online about the Supreme Court’s June 2026 ruling on deprivation of liberty. Some people are saying everything has changed overnight. Others are saying the Cheshire West “acid test” has gone completely and fewer DoLS applications will now be needed. It is understandable that this has caused confusion. The truth is more balanced than that. GOV.UK continues to host a Deprivation of Liberty Code of Practice page, published on 2 June 2026, describing the Code as the legal framework and safeguards for protecting individuals who may be deprived of their liberty under the Mental Capacity Act 2005.
Yes, this is an important legal ruling. Yes, it does change the way the law looks at deprivation of liberty. But no, it does not mean that care providers, managers or leaders should panic or suddenly stop thinking about safeguards. The Mental Capacity Act 2005 is still in place, and official sources still show that DoLS remains part of the legal framework in England and Wales. Legislation.gov.uk continues to show the Mental Capacity Act 2005 as current legislation, and the Local Government Association still states that DoLS continues to be the mechanism for authorising a deprivation of liberty for adults aged 18 or above in hospitals and care homes.
This article explains what happened, why people are talking about it, what the Court decided, and what it really means for practice right now. It is written for care providers, managers, leaders and practitioners who want clarity rather than panic.
What was this case actually about?
This case came from Northern Ireland and went to the UK Supreme Court. The question was whether a person aged 16 or over who lacks capacity to make decisions about their care and treatment could still be treated as giving valid agreement to their living arrangements through their wishes and feelings. In simple terms, the Court was asked whether someone could be seen as accepting their care arrangements even if they did not have mental capacity in the usual Mental Capacity Act sense. The official Supreme Court case page sets out that issue clearly.
The official Supreme Court case page says the issue was whether the Northern Ireland Minister of Health had the power to revise the local Deprivation of Liberty Safeguards Code so that people who lack capacity could still give valid consent to confinement through the expression of their wishes and feelings. The case page also confirms that this issue was being considered against the background of the earlier Cheshire West ruling. If you want to read the official documents for yourself, the key sources are the Supreme Court case page, the GOV.UK Deprivation of Liberty Code of Practice, and the Mental Capacity Act 2005.
Why was Cheshire West so important before this ruling?
Before this new decision, many practitioners worked from the well-known Cheshire West acid test. In simple terms, the test asked whether the person was under continuous supervision and control and not free to leave. If those things were present, and the person lacked capacity to consent to the arrangements, that was likely to amount to a deprivation of liberty. The Supreme Court case page itself summarises the earlier Cheshire West position by saying that Article 5 of the Human Rights Act applied even where the person who lacked capacity appeared content with the arrangements for their care and treatment.
That older approach gave providers and local authorities a relatively clear framework, even if many people felt it had become too blunt and too broad in practice. The Local Government Association still describes DoLS as the current mechanism for authorising a deprivation of liberty in hospitals and care homes for adults aged 18 and over, which shows how deeply the Cheshire West way of thinking has shaped practice over the last decade.
What did the Supreme Court decide in 2026?
This is the key part.
A published summary by 39 Essex Chambers explains that the Supreme Court determined that the Cheshire West acid test for identifying the objective part of deprivation of liberty was wrong and had moved away from European case law. The summary says the Court decided that deprivation of liberty should not be identified by a single bright-line test alone, but by looking at the person’s overall situation in a more detailed and individual way.
The same summary explains that the Court returned to a multifactorial approach. That simply means looking at a range of factors rather than relying on only one or two questions. Those factors include the degree of control over the person, whether they can leave, the effect of the restrictions on them, how long the restrictions last, whether they object, whether there is coercion (pressure or force), and how normal or restrictive the setting is for that person.
The Court also said something else that has caused a lot of debate. According to the summary, the Court treated “valid consent” under Article 5 as a separate legal idea from the usual Mental Capacity Act test for capacity. In plain English, the Court said that a person might not have capacity to make a care decision under the Mental Capacity Act, but might still be able to show enough understanding and acceptance of their situation for Article 5 purposes. That is a big legal development. It is one of the main reasons people are saying this is such an important ruling.
So, has everything changed overnight?
This is where it is important to slow down and be careful.
The legal test has changed immediately. The Supreme Court has overruled Cheshire West as the governing approach and said that deprivation of liberty must now be assessed using a multifactorial approach, looking at the individual’s specific situation and the full circumstances of the restrictions in place. The official judgment explains that the meaning of deprivation of liberty in the Mental Capacity Act 2005 is directly linked to Article 5 of the European Convention on Human Rights, so this new interpretation matters straight away.
At the same time, the wider Mental Capacity Act 2005 and DoLS safeguards framework have not disappeared. The Mental Capacity Act remains in force, and official sources still describe DoLS as the mechanism for authorising deprivation of liberty in hospitals and care homes for adults aged 18 and over. GOV.UK continues to host a Deprivation of Liberty Code of Practice page, and the Local Government Association still says that DoLS continues to be the mechanism in those settings.
So the clearest way to understand the position is this: the legal definition and trigger have changed immediately, but the wider safeguards system still exists. Providers should not keep using Cheshire West as though nothing has happened, but nor should they assume that all safeguards have fallen away. The law has changed first; guidance and practice systems will take time to catch up.
What does this mean for care providers and managers right now?
Right now, this ruling should still be a prompt for careful thinking, not panic.
What has changed is the legal lens through which deprivation of liberty must now be viewed. Providers should no longer rely on the old Cheshire West acid test alone. The Supreme Court has said the assessment must now be broader and more individual, looking at the person’s situation as a whole. The official judgment explains that deprivation of liberty must be approached by considering all three elements of the Article 5 test together, and the published summary prepared by 39 Essex Chambers explains that the Court has returned to a multifactorial assessment based on the individual’s concrete situation.
What has not changed is the need to act lawfully and keep safeguarding at the centre of practice. The DoLS authorisation framework still exists in the settings where it currently applies, and the Local Government Association still states that DoLS continues to be the mechanism for authorising deprivation of liberty in hospitals and care homes for adults aged 18 and over.
So the practical message should be balanced and reassuring: do not ignore the ruling, but do not rush into blanket changes either. The sensible short-term response is to recognise that the legal test has shifted now, while continuing to use the current safeguards framework lawfully and making sure that wishes, feelings, objection, distress, coercion and restrictions are clearly recorded.
Does this mean providers can stop applying for DoLS if someone seems happy?
This is one of the biggest misunderstandings, and it is exactly where careful wording matters.
The Supreme Court has said that a person’s wishes, feelings, acceptance and lack of objection can now be relevant in a way that Cheshire West treated differently. The 39 Essex Chambers summary says the Court has recognised that a person who lacks legal capacity under domestic law may still be capable of giving valid consent for Article 5 purposes, depending on their level of awareness and acceptance of the arrangements. The official judgment itself explains that the proposed revised code was intended to allow some people who lack mental capacity under domestic law to still be treated as capable of giving valid consent through the expression of wishes and feelings.
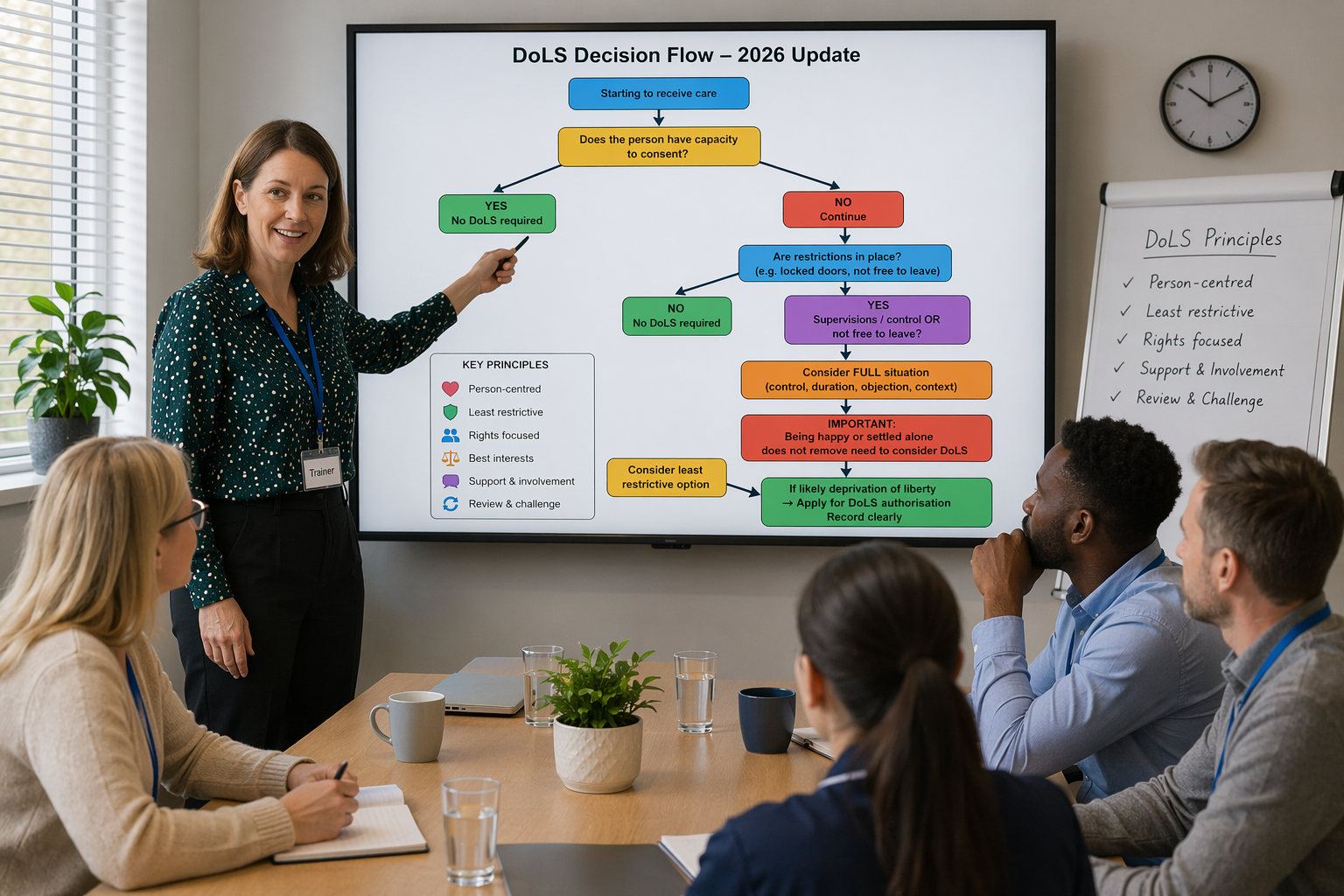
However, that does not mean that providers can now simply say, “They seem happy, so no DoLS is needed.” The correct position is more careful than that. Cases now need to be assessed under the new multifactorial legal approach, not under the old acid test alone. If, after applying that wider approach, the case is still likely to amount to a deprivation of liberty, then the DoLS framework remains the route for authorisation in the settings where it currently applies.
So the practical message is this: being happy or settled is now relevant, but it is not a shortcut. It is one factor in the wider legal picture. Providers should be cautious, avoid blanket assumptions, and make sure that wishes, feelings, objection, distress, coercion and restraint are clearly recorded while guidance develops.
What about Liberty Protection Safeguards?
This ruling also lands at a time when reform was already being discussed.
A 2025 GOV.UK press release said the government planned to launch a consultation in 2026 on Liberty Protection Safeguards, describing the current DoLS system as bureaucratic and complex and saying the new safeguards were intended to improve protection and reduce backlog. That press release also linked the reform conversation to the Supreme Court’s review of what counts as a deprivation of liberty.
That does not prove this Supreme Court ruling will immediately change the law again and Liberty Protection Safeguards have now been brought in. But it does show that wider reform was already on the agenda before this judgment.
In Summary
If you only take one thing from this blog, let it be this:
The Supreme Court has changed the legal test for deprivation of liberty with immediate effect. Cheshire West is no longer the governing test on its own. From now on, deprivation of liberty has to be looked at in a more individual, wider and more contextual way.
That does not mean the Mental Capacity Act and DoLS framework have disappeared. The wider safeguards system still exists, and DoLS remains the mechanism for authorising deprivation of liberty in hospitals and care homes for adults aged 18 and over. What has changed is the way we decide whether a case actually reaches that threshold in the first place.
So the real message is this: the trigger has changed immediately, the wider safeguards framework remains, and providers now need to assess cases using the new multifactorial approach rather than relying on the old Cheshire West acid test alone.
Why this matters to us as trainers
We have been delivering Mental Capacity Act and DoLS training for a significant amount of time, and one of the things we have always emphasised is that good practice should never be reduced to a blunt, one size fits all formula. Our training has consistently reflected an individualised, person-centred approach, helping providers and leaders think beyond tick-box thinking and really understand how capacity, best interests, restrictions and safeguarding work together in day to day practice.
In many ways, that is why this ruling is so interesting. It does not mean that everything changes overnight, but it does suggest that the law is moving in a direction that many good practitioners have already been aiming for: a fuller, more personalised way of understanding deprivation of liberty, rather than relying only on a rigid standard test. If you would like to explore that in more detail, including how this ruling fits into the current Mental Capacity Act and DoLS framework, you can find details of our training here: Mental Capacity Act Training for Leaders & Managers
Many people who attend our training say that it helps them make sense of the Mental Capacity Act in a practical, straightforward and much more confident way. If your team needs calm, clear and balanced support around Mental Capacity Act practice, DoLS, or safeguarding for leaders and managers, this is exactly the kind of discussion we cover in depth.

Quick FAQs
Has DoLS changed in 2026?
The Supreme Court has changed the legal test for deciding whether someone is deprived of their liberty, and that change takes effect immediately. However, the wider Mental Capacity Act and DoLS safeguards framework still exists, and DoLS remains the authorisation mechanism in hospitals and care homes for adults aged 18 and over.
What should providers do now?
The legal analysis has changed because the Supreme Court has overruled the old Cheshire West approach as the sole test, but official sources still show a live DoLS framework in England and Wales.
Did the Supreme Court overturn Cheshire West?
Yes. Legal summaries published after the decision describe the Supreme Court as having overruled Cheshire West.
Do I still need to think about safeguards?
Yes. The ruling changes the legal definition and trigger, but it does not remove the wider safeguarding framework. GOV.UK still describes the Deprivation of Liberty Code of Practice as setting out the legal framework and safeguards, and the Local Government Association still says that DoLS continues to be the mechanism in hospitals and care homes for adults aged 18 and over.
If someone seems happy or settled, does that automatically mean no DoLS is needed?
No. The Supreme Court has said that wishes, feelings, acceptance and lack of objection can be relevant to the legal assessment, and a person may in some cases be able to give valid consent for Article 5 purposes even if they lack legal capacity under the Mental Capacity Act. But that does not mean providers should treat apparent contentment as the whole answer. Cases now need to be assessed using the new multifactorial approach, and where the threshold is still met, the DoLS framework remains the route for authorisation in the settings where it applies.
What is the biggest practical message for care leaders?
Do not panic. Focus on person-centred, least restrictive practice, clear decision-making, and understanding the individual’s circumstances in a fuller way. The law is moving toward a more individual approach, but the current legal framework still matters.
Do providers need to rewrite all their policies immediately?
Not necessarily. The official sources confirm that the legal test has changed immediately, but they do not set out a mandatory immediate policy rewrite process. A balanced response is to review how deprivation of liberty is being identified and recorded, while waiting for clearer guidance to emerge.
Final thought
For me, this ruling is not a reason for fear. It is a reason for reflection.
It suggests that the law is moving away from a blunt, rigid formula and toward a more personalised way of understanding deprivation of liberty. In many ways, that is what good care should have been doing all along. But it also means we need to stay balanced, lawful and careful while the sector works through what this ruling means in practice. The safest message for providers right now is not panic, not oversimplification, and not bandwagon thinking. It is calm, thoughtful, person-centred practice grounded in the current legal safeguards that still exist today.